Knee Osteoarthritis and Platelet Rich Plasma
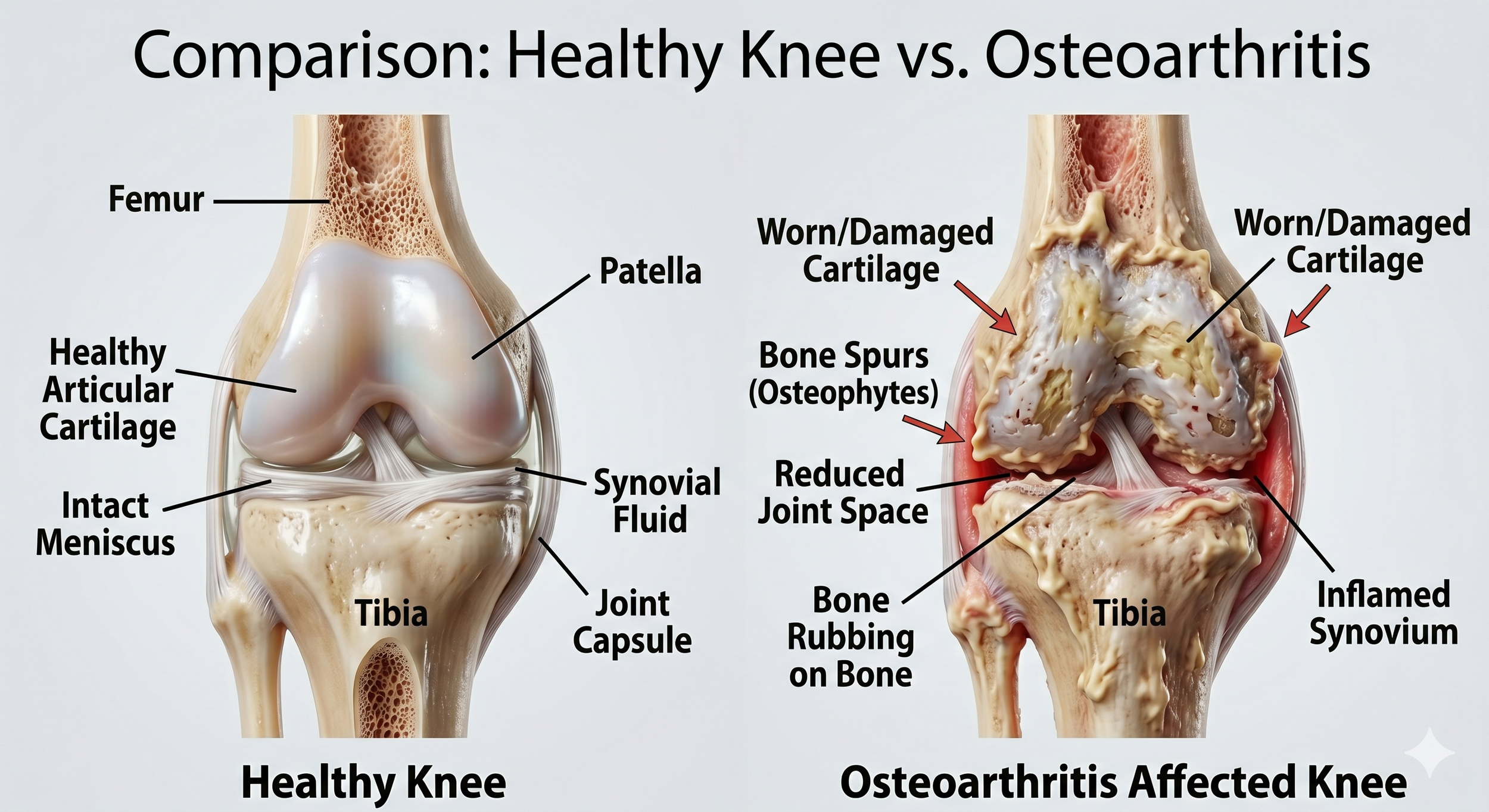

Knee arthritis is a mechanical and degenerative condition with limited disease-modifying options.
While structured physical therapy and weight management remain cornerstones of long-term management, many patients will find themselves in the uncomfortable ‘gray zone’ of a knee that is slowly declining in function and increasing in pain, but not so significantly that a knee replacement is warranted. For this reason, many patients feel stuck in a physical limbo of sorts - unable to move forward with a sustainable treatment option.
Anti-inflammatories such as ibuprofen or naproxen may provide symptomatic relief, but for many, the potential side-effects of GI, cardiac and kidney toxicity begins to outweigh the benefit. Alternatively, intra-articular corticosteroids - aka ‘cortisone shots’ - may provide quick relief for weeks to months, but over time, repeated injections have been associated with concerns for accelerating cartilage degradation.
Platelet rich plasma (PRP) injections can be the bridge many patients are looking for.
PRP introduces supraphysiologic concentrations of growth factors (PDGF, TGF-β, IGF-1, VEGF) directly into the joint environment. The proposed mechanisms include synoviocyte modulation, suppression of catabolic cytokines (IL-1β, TNF-α), chondrocyte stimulation, and improved synovial fluid viscosity - ALL of which contribute to a treatment modality that not only outperforms corticosteroid injections at the 6 month mark, but also may be associated with long-term protection of cartilage.
References
- Dai W, et al. A systematic review of platelet-rich plasma use in foot and ankle surgery. Ann Transl Med. 2021;9(1):66. — Supports superiority of PRP over HA for pain and function in early-to-moderate knee OA.
- Shen L, et al. The temporal effect of platelet-rich plasma on pain and physical function in the treatment of knee osteoarthritis: systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res. 2017;12(1):16. — Demonstrates PRP benefit concentrated in KL 1–3; attenuated in advanced disease.
- Kon E, et al. Platelet-rich plasma: intra-articular knee injections produced favorable results on degenerative cartilage lesions. Knee Surg Sports Traumatol Arthrosc. 2010;18(4):472–479. — Early RCT establishing 6–12 month functional benefit and need for repeat dosing.
- Laudy ABM, et al. Efficacy of platelet-rich plasma injections in osteoarthritis of the knee: a systematic review and meta-analysis. Br J Sports Med. 2015;49(10):657–672. — Meta-analysis confirming PRP superiority over saline and HA at 6 months for pain reduction.
- Filardo G, et al. Platelet-rich plasma: why intra-articular? A systematic review of preclinical studies and clinical evidence on PRP for joint degeneration. Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2459–2474. — Reviews preparation heterogeneity and calls for standardized protocols; highlights LP-PRP vs L-PRP distinction.
- Forogh B, et al. Intra-articular platelet-rich plasma injections versus intra-articular corticosteroid injections for symptomatic management of knee osteoarthritis: systematic review and meta-analysis. BMC Musculoskelet Disord. 2021;22:487. — Meta-analysis of 8 RCTs (648 patients) showing PRP significantly outperforms corticosteroid for pain, stiffness, and function at 3, 6, and 9 months; superior outcomes sustained at 12 months; greatest effect at 6 months.
- Bansal H, Leon J, Pont JL, Wilson DA, Bansal A, Hyder I, Preoteasa I. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Sci Rep. 2021;11:3971. — RCT of 150 patients demonstrating that an absolute count of ≥10 billion platelets is required for sustained chondroprotective effect at one year in moderate knee OA; PRP group showed significant improvements in WOMAC, IKDC, and 6-minute walk distance vs. HA, with significant reductions in IL-6 and TNF-α at one month.
This summary is intended for educational purposes. Evidence quality and clinical recommendations continue to evolve. Clinicians should consult current literature and exercise individualized clinical judgment.